
The Forgotten Biliary Stent
Pathophysiology, Surgical Retrieval, and Lavage-Related Complications
Author
Dr. Ashish Kumar Ohri
Consultant Surgeon
Arogya Hospital, Ludhiana (Punjab, India)
📞 9815550159
✉️ ashishohri@gmail.com
1. Introduction: When a Temporary Device Becomes a Permanent Problem
Endoscopic biliary stenting via ERCP is a cornerstone in managing obstructive jaundice arising from benign or malignant biliary strictures. Plastic biliary stents are intentionally designed as temporary devices, with recommended exchange or removal within 3–6 months. Failure to adhere to this timeline converts a therapeutic tool into a pathological foreign body—commonly termed a forgotten or retained biliary stent.
Unlike acute biliary obstruction, retained stents may remain clinically silent for extended periods due to the wicking phenomenon, where bile continues to flow around an occluded lumen. This deceptive drainage delays presentation while allowing progressive pathological changes: bacterial biofilm maturation, dense encrustation, stent fragmentation, migration, and ultimately formation of a stentolith.
When symptoms do emerge, they are often severe—acute cholangitis, sepsis, or secondary biliary cirrhosis. At this stage, conventional endoscopic retrieval frequently fails, necessitating surgical salvage, most commonly via Laparoscopic Common Bile Duct Exploration (LCBDE). This transition introduces additional risks, including the under-recognized but critical complication of lavage-induced hydrothorax through diaphragmatic defects.
2. Biliary Stent Design and the Seeds of Failure
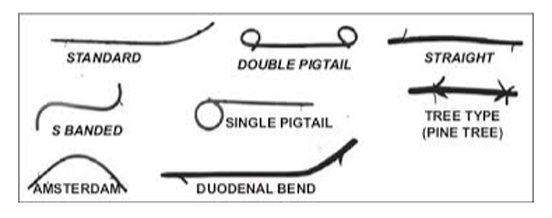
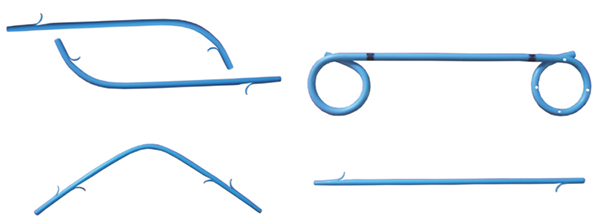
Plastic biliary stents are typically manufactured from polyethylene or polyurethane and are available in straight or pigtail configurations, commonly sized 7Fr or 10Fr. While cost-effective and easy to deploy, their fixed narrow lumen (≈2–3 mm) predisposes them to obstruction.
Protein adsorption begins immediately after placement, initiating sludge deposition and bacterial adherence. Side holes, flaps, and barbs—designed to prevent migration—paradoxically increase turbulence and biofilm anchoring.
Clinical studies consistently demonstrate a steep decline in plastic stent patency beyond three months, underscoring why delayed follow-up is not a benign oversight but a predictable failure point.
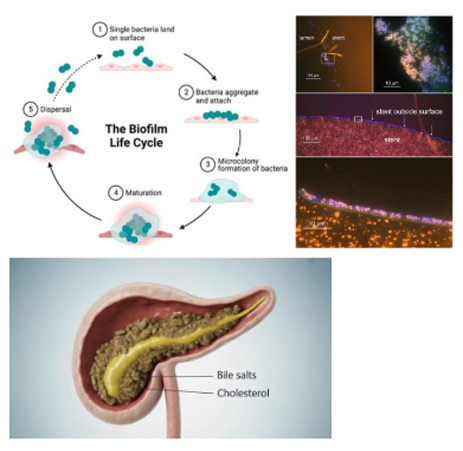
3. Biofilm Formation and the Evolution to Stentolith
3.1 Conditioning Film and Bacterial Colonization
Once placed, the stent surface is rapidly coated with host proteins—albumin, fibrinogen, and biliary glycoproteins—forming a conditioning film. This layer facilitates adhesion of ascending enteric bacteria such as E. coli, Klebsiella, Enterococcus, and Pseudomonas.
These organisms transition from planktonic forms to organized biofilms by secreting an extracellular polymeric substance (EPS) matrix. This matrix protects bacteria from antibiotics and traps biliary constituents.
3.2 Wall Shear Stress and Encrustation Physics
Biofilm proliferation is governed by wall shear stress (WSS). Moderate bile flow optimizes nutrient delivery without disrupting bacterial adherence, promoting maximal biofilm growth. Over time, enzymatic deconjugation of bilirubin leads to calcium bilirubinate precipitation, progressively mineralizing the biofilm.
3.3 Stentolith: The End Stage
Unchecked encrustation transforms the stent into the core of a large pigment stone—a stentolith. These complexes may reach several centimeters, fully encasing the stent and fixing it to the bile duct wall, rendering endoscopic extraction hazardous or impossible.
4. Mechanical Complications: Migration, Fracture, and Vascular Injury
4.1 Proximal Migration
Proximal stent migration occurs in up to 10% of cases and is more common in benign strictures, dilated ducts, straight stents, and long indwelling durations. Migrated stents may lodge at the hepatic confluence, frequently embedded within stone or hyperplastic tissue.

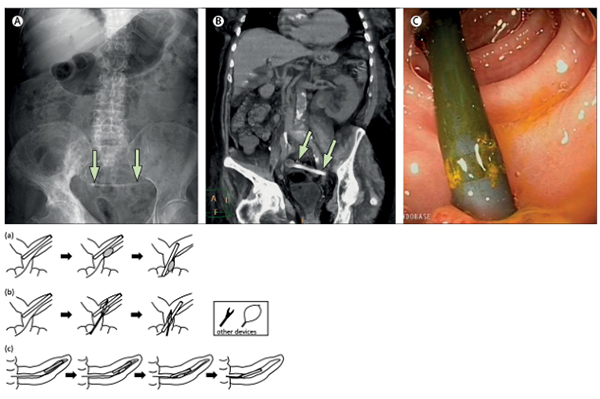
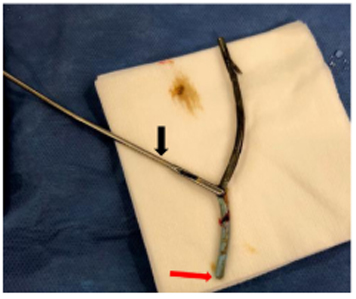
4.2 Stent Fracture
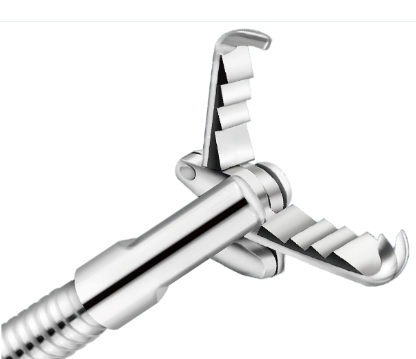
Chronic exposure to bile acids and bacterial enzymes leads to polymer embrittlement. During attempted ERCP removal, the stent may fracture—often at side holes—leaving proximal fragments without a retrieval handle.
4.3 Portal Vein Fistula
In rare but catastrophic cases, chronic pressure erosion allows a migrated stent to fistulize into the portal vein, presenting as hemobilia, hemorrhagic shock, or sepsis. Endoscopic traction in such cases can be fatal; definitive management is surgical.
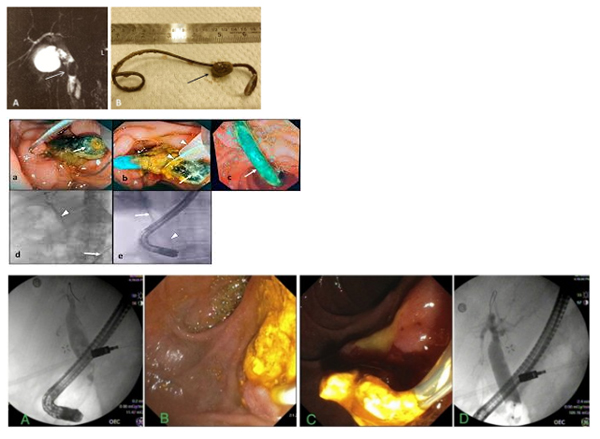
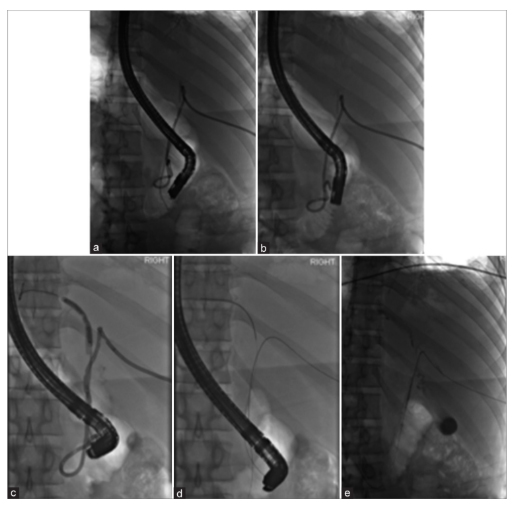
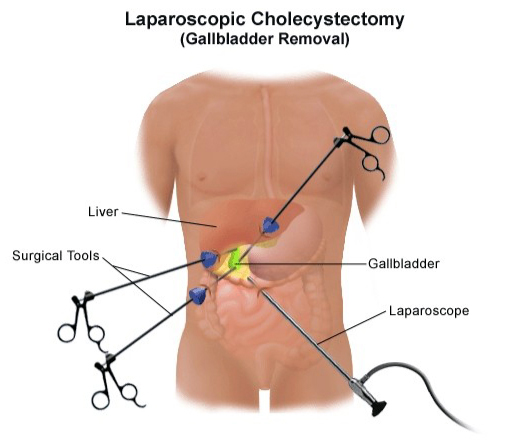
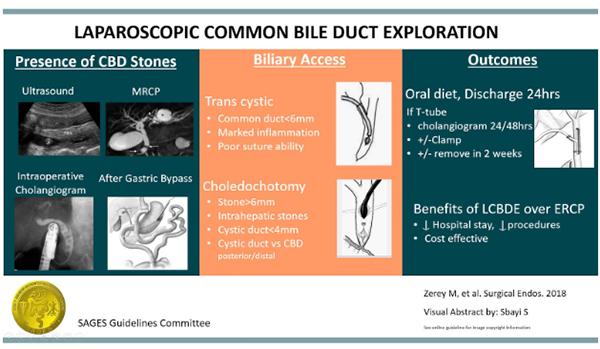
5. Surgical Salvage: Laparoscopic Common Bile Duct Exploration
When ERCP fails or is unsafe, LCBDE provides definitive single-stage management, often combined with cholecystectomy.
5.1 Why Choledochotomy Is Required
The transcystic route is usually impractical for intact retained stents due to their length and rigidity. A longitudinal choledochotomy allows controlled extraction and complete ductal inspection.
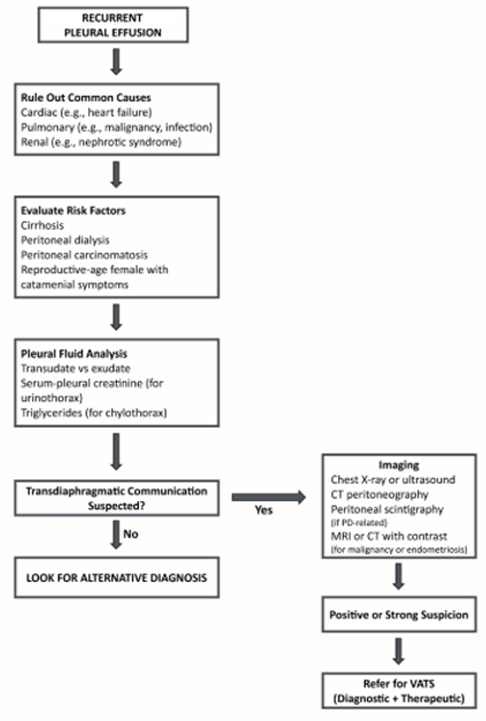
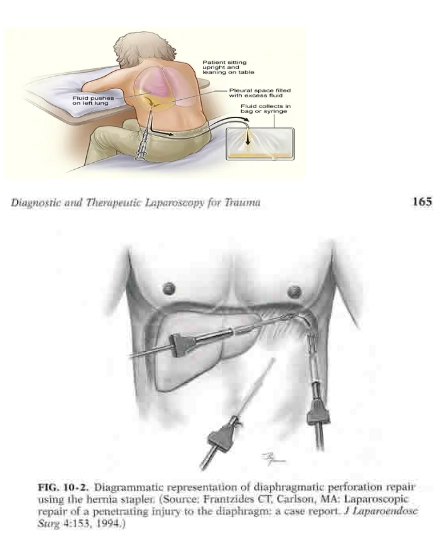
6. Lavage-Induced Hydrothorax: The Hidden Intraoperative Threat
During biliary surgery, copious saline irrigation is routinely used to clear infected bile and debris. In susceptible patients, this may precipitate acute hydrothorax via Porous Diaphragm Syndrome (PDS).
7. Conclusion
Forgotten biliary stents represent a preventable yet potentially catastrophic complication of endoscopic therapy. Prevention through patient education and follow-up remains paramount. When neglect occurs, safe management demands surgical expertise, anticipation of complications, and meticulous intraoperative technique.